Chapter 16 in the R.M. Dolin book, “Truth and Trust in Crisis,” 2021
How does the COVID crisis end given the virus is with us forever and no one in government, media, or the medical profession is capable of responsibly discussing acceptable death rates, virial attenuation, herd immunity, or the efficacy of mandates. Conversations around reasonable risk have been canceled as open scientific debate is stifled and STEM communities abdicate responsibilities leaving each of us to act on personal utilities based on observations, experiences, and falsified data. Societies historically find ways to set acceptable utility for calamities like flu, airline accidents, car crashes, cancer caused by smoking, opioid overdoses, etc., but society has never dealt with a crisis driven more by narratives than calamity.
Through simple and creative analyzes we’ve demonstrated the extent of COVID’s perfect storm of unintended digital age consequences, including doctor data falsification, politician’s lust for power, government’s ability to exert control, media message manipulation, and our willingness to do whatever we’re told even when it defies logic or goes against what’s in our best interest. It’s become increasingly clear society won’t return to normal until crisis villains find ways to fend off claims they panicked, overreacted, and overreached.
We’ll only be allowed to live without viral worry after politicians and their willing cohorts are vindicated and we become numb to hysterically hyperbolic propaganda. Until then, we languish in various forms of social mandates and medical experiments while experts work tirelessly to invent new distractions like asserting that obviously attenuated COVID mutations “will kill us all.” We’ll be forced to fester in pandemic purgatory for the foreseeable future because politicians and government bureaucrats can’t conceive a convincing a way out of the crazy corner they panicked themselves into.
If only there was some magic elixir to rescue the moment; sure, we’d have to wait patiently for one that at least pretends to work, but once released and we’re all simultaneously inoculated, the virus is vanquished, and we’re permitted to return to our pre-COVID lives. The best part is we can take the magic elixir without worry or risk because government and trusted medical professionals will assure such a miracle potion can be safely developed at “warp speed.”[1]
The problem with this Pollyanna portrait is that while coronaviruses have existed for hundreds of years, an effective coronavirus vaccine has never been developed.[2] Ian Frazer, who developed the vaccine for human papilloma virus, asserts coronavirus vaccines are historically hard to make safe because the virus infects the upper respiratory tract, which human immune systems are not great at protecting. Fazer warns “If a vaccine elicits an immune response that misses the target cells, the result could potentially be worse than if no vaccine was given.”[3]
This is not to suggest vaccines aren’t important, in fact, they’re essential. As hard as it may be to believe, 1.5 million children die each year from vaccine-preventable illnesses[4]. The history of how vaccines came about is remarkable, it began in 1757 when Edward Jenner of England observed that cow-maids didn’t die from smallpox. He started testing various hypotheses, eventually going macabre by intentionally infecting a young boy first with cowpox, then with smallpox; luckily for the boy, things work out. By 1796, Jenner had the world’s first vaccine[5], although it still takes 200 years to eradicate smallpox.
In the early 1800s, French scientist Louis Pasteur, who’s most known for pasteurization, develops a process to produce vaccines in a laboratory. In the early 1950’s, American scientist Jonas Salk[6] develops the technique of injecting people with a mild strain of an illness as a form of vaccination against that illness. He used this technique to vaccinate children for polio starting in 1955, and forty years later polio has been mostly irradicated. The annual flu shot is based on Salk’s platform of injecting you with the flu to prevent you from getting the flu.
It’s impressive how the world goes from taking 200 years to eradicate smallpox to 40 years to eradicate polio to now being on the precipice of conquering a deadly virus whose eluded eradication for centuries with one decisive blow: an Operation Warp Speed goal requiring scientific breakthroughs worthy of Nobel Prizes. Imagine going from pretrial development to complete eradication in under a year; something that usually takes decades of research, careful studies, and controlled trials. Of course, accomplishing this requires some risk and perhaps cutting a few corners but all within the margins of acceptable utility.
Suggesting a coronaviruses vaccine can be developed at “warp speed,” is of course marketing-speak for outside established protocols and even the head of the government’s Operation Warp Speed Task Force, does not believe this can be accomplished.[7] This begs the overriding question society as a whole, and you as an individual, must address: once our vaccine’s been rushed through development, production, and distribution, and you’re assured it’s safe and effective even though no field trials are performed, should you take it? Before answering, assume the vaccine will be based on Jonas Salk’s fully vetted technique of injecting you with COVID to protect you from getting COVID. Also, recall the medical disaster that resulted from rushing Thalidomide[8] into mass distribution in the 1960’s only to give thousands of children horrific birth defects.
Imagine the WWII-style propaganda campaign that’ll be rolled out to coincide with our warp speed inoculation; beautiful Hollywood celebrities’ touting this newly developed cure as the miracle of our age that once everyone takes, magically teleports us back to a pre-COVID world where Ward and June Cleaver are comfortable once more allowing Wally and Beaver to go outside. An inconvenient reality that will unfortunately be overlooked is even after taking the magic elixir, COVID caused deaths will continue because, virus vaccines are never effective; we still get flu after taking the flu vaccine. The good news is that after we’re all inoculated, we can take off our masks, return to our restaurants, and walk our streets without worry; at least that’s what the marketing campaign with complicit celebrities will promise.
The best part of their propaganda that won’t be mentioned is that the vaccine doesn’t even have to work. Six months from now when our fearless leaders triumphantly declare victory over COVID, the nation can collectively exhale. By then the CDC will have ratcheted their death count numbers down to actual levels, governors will give grand speeches pontificating the wisdom and effectiveness of their leadership, and schools will reopen. Yes, boys and girls, moms and dads, the idyllic American dream will once again power our great nation, and the best part is that even if the vaccine is nothing more than a placebo, it’s still every bit a cure because, what the marketing campaign fails to mention, but some scientists have been trying to point out, is that coronavirus vaccines don’t work, at least not to the levels of efficacy that will be touted.
If our vaccine where to come with an entirely new, revolutionary, and untested delivery platform, say one altering your DNA in ways that make you miraculously impervious to coronaviruses, then skeptical scientists would be forced into silence because there’s no place for science in a magic show. This crisis has demonstrated it’s not hard to get the medical and science communities to acquiescence to whatever’s required to advance necessary narratives.
In our eagerness to resume normal life, we’ll acquiesce to minor but necessary modifications to our DNA, after all, taking the nonvaccine vaccine is a small ask for finally being able to crawl out from under COVID constrictions. Keep in mind, one utility of vaccination is that it accelerates the rate at which we reach herd immunity and COVID becomes naturally benign. So, if they give everyone COVID to keep anyone from getting COVID as a Jonas Salk based vaccine platform would do, or they alter our DNA so we’re genetically not suspectable to coronaviruses, we reach heard immunity instantly and the nonvaccine vaccine appears effective. Either way, it’s fascinating how fate finds a way through its maze of unintended consequences.
Given the anticipated controversy surrounding any COVID vaccine, I’m compelled to disclose up front that while I am a scientist and therefore a skeptical of all breakthrough technologies, I’m also a vaccine advocate; and this after taking the Typhoid vaccine before going to Central American and then getting Typhoid. Given Typhoid has a 20% death rate, it was not a fun week and the only thing that saved me was repeated vodka sponge baths and massive doses of pure penicillin available at the island pharmacy. Conversely, I got the smallpox, tuberculosis, hepatitis, tetanus, etc. vaccines, and haven’t gotten those diseases and, somehow managed to turn out mostly alright.
Remember when experts told us cholesterol in eggs could kill? That was of course before they decide eggs are packed with essential proteins that promote brain function, weight loss, and cell regeneration. Remember when coffee caused cancer, before finding out it doesn’t. Health warnings from “experts” come and go as fast as fad-diets, or at least as fast as academic funding streams change.
COVID’s certainly come with its cohort of crazy concerns. During our early innocence a well-paid study convinced us ibuprofen caused certain COVID death, so we all hoarded acetaminophen. Big tobacco was orgasmic when university researchers on retainer declared smoking cigarettes was not a preexisting condition because nicotine prevents COVID. Imagine the salivating at corporate tobacco over the prospect of addicting 320 million Americans to cigarettes or other nicotine enhanced products in our hysterical bid to stave off death.
As zany as these absurdities seem, such speculation is an essential part of inventive science that begins with an observation and leads to hypothesis testing. Perhaps the most widely publicized example of this during COVID involved the use of Chloroquine Hydrochloride[9], which started with epidemiologists observing COVID’s inability to gain a toehold in countries where malaria vaccinations are prevalent. That initial observation is followed by healthcare workers observing that patients taking chloroquine hydrochloride for arthritis fare better against COVID than other patients. From these valid observations, scientists in France begin experimenting and soon scientists in other countries are conducting experiments. The general conclusion, which unfortunately was highly politicized, indicates that while the drug may not be a silver COVID bullet, it may offer effective treatment for some patients. Studies have also found chloroquine hydrochloride can damage the heart and appears to have serious neurotoxic side effects (i.e., psychological disorders).[10] While passions concerning chloroquine hydrochloride’s efficacy remain high, we should agree it was good and right for scientists to investigate the drug’s potential based on observational evidence.
In science, more roads lead to dead ends than success but as Thomas Edison famously said, “Negative results are just what I want. They’re just as valuable to me as positive results. I can never find the thing that does the job best until I find the ones that don’t.”
As pharmaceutical companies rush to find COVID cures, the pressure to release vaccines without clinical trials is enormous and we’re assured it’s okay this one time. And why should we worry, in times of crisis vaccines development will surely be based on derivatives of vaccines used to treat previous coronavirus strains, like our annual flu shot based on Jonas Salk’s delivery platform. The health risk of developing a new vaccine platform without clinical trials is far too preposterous to ever be considered. That is unless the fine folks who engineered COVID were kind enough to also develop the antidote based on a new mRNA[11] platform that plays with our DNA.
As a vaccine advocate, I’m on board with a well-vetted Jonas Salk based vaccine that skips clinical trials, however, a new and unproven platform that screws with my DNA seems a bridge to far; I’d rather just get COVID and be done with the worry and hysteria, which I have been trying unsuccessfully to do for the past year. At the end of the day, I fear what this new and unproven mRNA protocol may do to my body more than I fear COVID, but as we discussed, each of us has our own utility function, which will lead to wide differentials on acceptable risk.
As the world contemplates a new vaccine platform that won’t be clinically trialed, let’s consider when this was previously done. A sedative drug in the early 1960’s called thalidomide[12] is prescribed to pregnant mothers to help with morning sickness. It’s enthusiastically endorsed and prescribed by doctors before being found to cause congenital malformation in children, i.e., deformities. My Mom thankfully resists pressure from her doctor to take thalidomide, even after being assured it’s safe. The thalidomide incident is a poignant reminder of what can go wrong when unproven drugs are rushed into mass distribution.
As pressure mounts to return to normal, so too does pressure to get some kind of vaccine developed and distributed as quickly as possible. Once released, the vaccine won’t roll out in stages, or even be voluntary, it will be simultaneously administered to the entire population as a condition for rejoining society. The question I’ve been wrestling with is should I get in line to receive this mandatory miracle or hole up until everyone else takes it? Once 70% of our population’s taken the vaccine and herd immunity is reached, COVID will be conquered, and I don’t need the vaccine.
Science is good but without proper control can be reckless. On my twelfth birthday, a cloud seeding experiment gets away from scientists in the Black Hills of South Dakota causing it to rain in unnatural ways. I’m living in Sturgis at the time, and a few miles east, it rains so hard that the dam in the canyon above Rapid City breaks, releasing a torrent wall of water that crashes through homes and buildings killing hundreds while leaving the flood plain in shambles.
In the aftermath, the Red Cross sets up mass vaccination centers where people line up. I don’t remember everything I get but remember walking down the center isle of a field hospital with both my little league shirt sleeves rolled over my shoulders so nurses could use these way-cool pneumatic guns to inject both arms with lifesaving drugs. The nurses were kind and committed, as all nurses are, and a particularly pretty nurse teasingly tells me after her needle goes deep into muscle that I won’t be throwing a baseball any time soon. I admit to being so impressed by the efficiency in which a small cadre of nurses can inject measured doses of multiple miracles to a large population in a very brief time, I never question the safety or efficacy of what’s being injected into me, after all, the hospital tent has a red cross painted on it and the nurses wear official looking white medical smocks.
That’s how I envision the mass COVID vaccination campaign being conducted; a medical truck rolls into town and everyone dutifully lines up as a cadre of committed nurses, sporting the newest injection gun technology, service us with optimized efficiency and effectiveness. And then we as individuals, as families, as communities, and as a nation wait and hope anticipated side effects are not too severe.
Buddha teaches that desire and suffering are two sides of the same coin. When the COVID cure finally comes, our entire population will be vaccinated all at once. Imagine, 320 million souls collectively flipping a COVID coin. On one side is an outcome where we’re allowed to return to our pre-COVID lives and on the flipside are the children of thalidomide. It’s an interesting choice we must make, one that ultimately comes down to a matter of truth, trust, and utility.
Epilogue: Let’s jump past our post-COVID vaccine era and listen to the U.S. Senate testimony of three Depart of Defense (DOD) whistle-blowers who claim the DOD falsified illness data to hide the negative ramifications that resulted from forcing all military personnel to get the COVID vaccine.[13] Their testimony asserts that DOD falsified pre-COVID health data to make vaccine side effects seem less dramatic.[14] Table 16.1 details what the whistleblowers assert are the true statistics of the mandatory COVID vaccine on our young health military demographic relative to pre-COVID statistics.
Table 16.1 Department of Defense Data on COVID Vaccine Side Effects as a Measure of Increases in Illness, Sickness, and Disease.
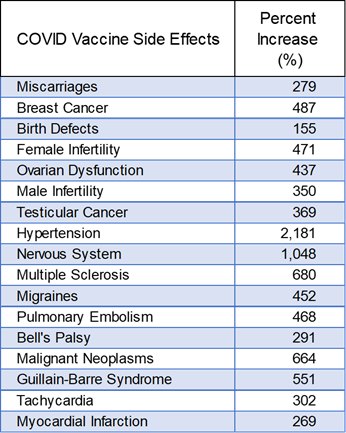
The three whistleblowers came forward to disclose deliberate efforts by the DOD to inflate previous years incidents of sickness and illness to make the 2021 post-vaccination data appear normal. From 2016 to 2020, the DOD average number of diseases and injuries reported per year was 2,045,556. In 2021, however, the year of vaccination, the rate increases to 21,512,583, which represents an increase of 1,053%, which the DOD allegedly covers up by inflating previous year’s data; a message manipulation similar to what goes on at CDC.
If these allegations are true, the children-of-Thalidomide will be eclipsed by the soldiers-of-COVID as our trust in government data is further diminished. One cause of concern leading me to believe there could be something to this is the manner in which the Senate testimony is dispositioned; instead of loudly debunking the assertions of the whistleblowers with hard evidence they’re wrong, the entire incident is quickly and quietly disposed of, and the whistleblowers vanish from the spotlight, something I find odd and concerning. Why aren’t prominent scientists and medical professionals lining up to debunk these claims? Why is the military not publicly defending themselves from these allegations? Why is the media so surprisingly quiet and why has all discussion on vaccine side effects been canceled?
Note: This chapter is based on a series of 2020 essays submitted to major media outlets, including the NY Times, Washington Post, and Chicago Tribune. The essays can be found at: https://rmdolin.com/commentary/
Read the entire “Truth and Trust in Crisis,” book.
[1] Trump unveils ‘warp-speed’ effort to create coronavirus vaccine by year’s end | Donald Trump | The Guardian
[2] Will There Be a Coronavirus Vaccine? Maybe Not (nymag.com)
[3] We’ve never made a successful vaccine for a coronavirus before. This is why it’s so difficult – ABC News
[4] Vaccines: What are they and how do they prevent disease? – Vital Record (tamhsc.edu)
[5] Smallpox vaccine – Wikipedia
[6] Jonas Salk | Biography, Facts, & Polio Vaccine | Britannica
[7] Pflanzer, L., “The head of Operation Warp Speed told us about his day that starts at 2:30 a.m. and shared his timeline for a coronavirus vaccine in an exclusive interview,” Business Insider, August 21, 2020.
[8] History of Thalidomide (news-medical.net)
[9] Quarantine Day 21: Zinc, Quercetin, and a Curious Minded Engineer – An Engineer’s Perspective (rmdolin.com)
[10] FDA Warns Hydroxychloroquine, Chloroquine Should Only Be Used By Doctors As Drugs Could Have Life-Threatening Side Effects (newsweek.com)
[11] Understanding mRNA COVID-19 Vaccines | CDC
[12] What is thalidomide? | Thalidomide
[13]https://www.realclearpolitics.com/2022/01/27/dod_data_reveals_surges_in_covid_vaccine_adverse_events_561704.html
[14] Horowitz: The Pentagon’s RESPONSE to the explosive DOD medical data is an even bigger story than the data – TheBlaze
