Chapter 11 in the R.M. Dolin book, “Truth and Trust in Crisis.”
In response to COVID, states across the nation implement varying forms of quarantine; first to flatten the curve ahead of Armageddon Day on April 14th and then to slow virus spread. As we move toward fall, people are beginning to question the efficacy of quarantines since they’ve done little to alter COVID’s outcome. Some are waking up to is the way lockdown states uniformly implemented the first “reverse-quarantine” in human history. One way to assess the efficacy of quarantines is to compare our COVID incarceration to the 2017 flu season; you recall that horrible year when we lived through fear and panic as 61,000 Americans died from influenza and government failed to implement any mitigation mandates.
Quarantine is defined as a precautionary period where those possibly exposed to a contagion undergo isolation to protect the healthy population and until COVID, quarantines have exclusively been used in this manner. An early example of quarantine comes from the Old Testament where lepers are isolated from the general population to avoid spreading disease. In the 14th century Venice establishes the first formal quarantine protocols to stave off the Black Death by requiring all ships entering port to quarantine for 40 days. During COVID, crisis managers invert century’s old protocols by isolating healthy populations and in psychotic states, like New York, intentionally infecting healthy populations.
America’s first official quarantine is at Bedloe Island in 1732 to isolate immigrants suspected of having smallpox or yellow fever. It’s ironically fitting that Bedloe Island eventually becomes home for the Statute of Liberty. In 1799, a special hospital is built in Philadelphia to isolate people suspected of being infected with yellow fever in response to an outbreak that kills 12% of city’s residents. To put that in perspective, COVID currently kills 1.2% of the people infected.[1] If COVID were to kill 12% of our population it would equate to 40 million deaths.
In 1878, Congress passes the National Quarantine Act to combat Cholera outbreaks, and place authority to quarantine citizens with the federal government. This federal government’s authority is further strengthened in the Public Health Service Act of 1944, and in 1967, the CDC takes over management of the nation’s quarantine policies. It’s interesting that during COVID, the federal government never imposes quarantines, except on people entering the country. Meanwhile, many states illegally enact quarantine measures and do so in a logically irrational way.
We should not only question the logic of COVID quarantine policies, but their effectiveness as well. Early in the crisis when we didn’t know what kind of virus consumed us, panic grew from fear and a justifiable abundance of caution. But then, like wildfire that becomes self-perpetuating, state governments become obsessed with the need to not simply reduce risk, but to eliminate it all together; something impossible to achieve. Given our daily dose of dire doom from bureaucrats, the media, and medical professionals it may be hard to accept our assertion that COVID quarantines far exceed the responses of equally deadly pandemics.
Table 11.1. 2020 COVID Crisis versus 2017 Flu Season Statistics.
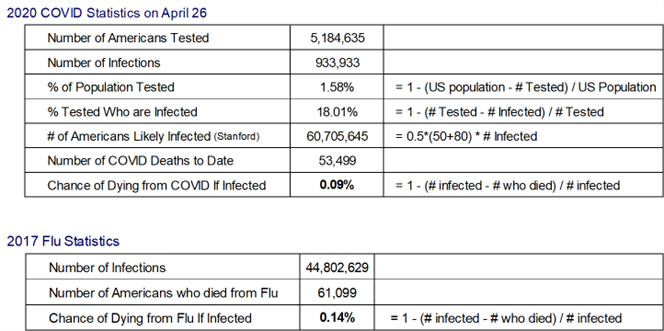
The data in Table 11.1 indicates the likelihood of dying from flu in 2017 was higher than the likelihood of dying from COVID. Why are the 61,099 flu deaths in 2017 not as precious as the 53,449 reported COVID deaths? The chance you die from flu once infected in 2017 was 1.6 times more likely than the chance of dying from COVID once infected yet not a single quarantine is established.
Throughout history, quarantines effectively isolated unhealthy populations to slow the spread of a disease, but it has never been shown to stop a disease’s spread and inverse-quarantines have never before been implemented. While quarantine measures are not instituted during the 2017 flu season, during what appears to be a less deadly COVID crisis, politicians decide rather than isolate at-risk populations to protect them, they’ll do the reverse defying not only logical reasoning but proven historical protocols.
Why invert established quarantine policy, and federal law? Is it possible crisis managers know something about COVID they’re reluctant to share, perhaps that it’s been engineered with a certain lethality they’re not at liberty to discuss? Why incentivize the falsification of data other than to justify draconian mitigation measures they irrationally seem committed to implement? While these are questions historical postmortems need to address, we limit our scope to the analysis of data as we find it.
We’ve discussed causal factors for why CDC data is inaccurately unreliable and how perhaps the only remaining way to ascertain the true impact of COVID is by utilizing actuarial data. We’ve previously demonstrated that through the first eight months of 2020, CDC death data tracks slightly below actuarial expectations. Let’s now consider causal factors for how such an outcome is possible, including
- Lockdowns lowered accident rates as fewer high-risk activities are permissible.
- Elective surgeries are delayed and doctor caused deaths average 440,000 per year.[2]
- Social isolation lowers flu deaths.
- Violent crime is reduced.
- Noncitizens return to their home countries.
At the same time, causal factors exist driving up the number of U.S. deaths, including
- Suicide rates are higher than expected.[3]
- Obesity, diabetes, heart ailments and other health related issues are exacerbated during lockdowns leading to higher than projected numbers of deaths.
- Child immunizations are delayed leading to increases in childhood deaths.
- Drug abuse increases, both legal and illegal.
These and other causal factors suggest it’s impossible the delta between pre-COVID expected deaths and actual deaths are COVID caused. However, in the aggregate fewer Americans are dying this year than expected before pre-COVID. It seems implausible to say that during a global pandemic of unprecedented proportion, the number of Americans who have died so far this year is 4,635 below pre-pandemic expectations.
Death is the last outcome of life, which means acceptable thresholds are required. We all want to be safe, even if we have different risk aversion utility functions. Actuarial evidence cannot measure the impact of quarantines on reducing COVID-caused deaths due to the many causal factors that come into play, and since the medical profession is falsifying data, we have no hope to ever quantify the efficacy of mitigation measures. However, Johns Hopkins University completed a study that suggests quarantines and mandates have minimal effect, which our actuarial analysis validates. Death data is easy to accurately measure as there is one overarching causal condition devoid of gradation, no longer being alive. What remains unknown are the causes of those deaths and in our digital age crisis, that information is both vital and unavailable.
Note: This chapter is based on a series of 2020 essays submitted to major media outlets, including the NY Times, Washington Post, and Chicago Tribune. The essays can be found at: https://rmdolin.com/commentary/
Read full “Truth and Trust in Crisis,” book.
[1] percent of population dying from COVID in US – Search (bing.com)
[2] How Many Die from Medical Mistakes in U.S. Hospitals? – Scientific American
[3] Bay Area sees ‘year’s worth of suicide attempts’ during shutdown: ‘Never seen numbers like this’ – Washington Times
