To see other COVID posts, visit my Quarantine blog.
Historically, quarantine has been used to isolate an unhealthy sub-population from a larger healthy population. Perhaps the earliest example of quarantine comes from the Old Testament where lepers were isolated from the general population to avoid spreading disease. It wasn’t however, until the 14th century that Venice established the first formal quarantine protocols to stave off the Black Death by requiring all ships entering port to quarantine for 40 days. In modern parlance, quarantine is defined as the precautionary isolation period that those possibly exposed to a contagion must undergo in order to protect the healthy population.
America instituted its first quarantine station in 1732 at Bedloe Island to isolate immigrants suspected of having small pox or yellow fever. Ironically, Bedloe Island is where the Statute of Liberty now resides. In 1799, a special hospital was built in Philadelphia to quarantine people suspected of being infected with yellow fever. This was in response to an outbreak that killed 12% of the city’s residents.
In 1878, Congress passed the National Quarantine Act to help combat Cholera outbreaks, which placed the authority to quarantine American citizens with the federal government. Final federalization occurred in 1921 after the deadly Spanish Flu pandemic. The federal government’s authority to quarantine was further strengthened in the Public Health Service Act of 1944, but it wasn’t until 1967, that the CDC took over management of the nation’s quarantine measures.
Not only are the state quarantines currently enacted during COVID illegal, they run contrary to the logical approach taken by countries and cultures reaching all the way back to the biblical era. In what seems like racing up the down staircase, the current COVID implementation of quarantine is predicated on isolating the healthy population, which is both unprecedented and illogical.
Not only does one have to question the logic of the COVID quarantine, one has to question its necessity. Early on in the COVID crisis when WHO and CDC didn’t know what kind of virus they were dealing with, a panic grew out of fear and a justifiable abundance of caution. But then like a wildfire that’s become self-consuming, state and federal governments across the globe were consumed by a need not just to reduce risk, but to eliminate it all together; something that is equally unprecedented and impossible.
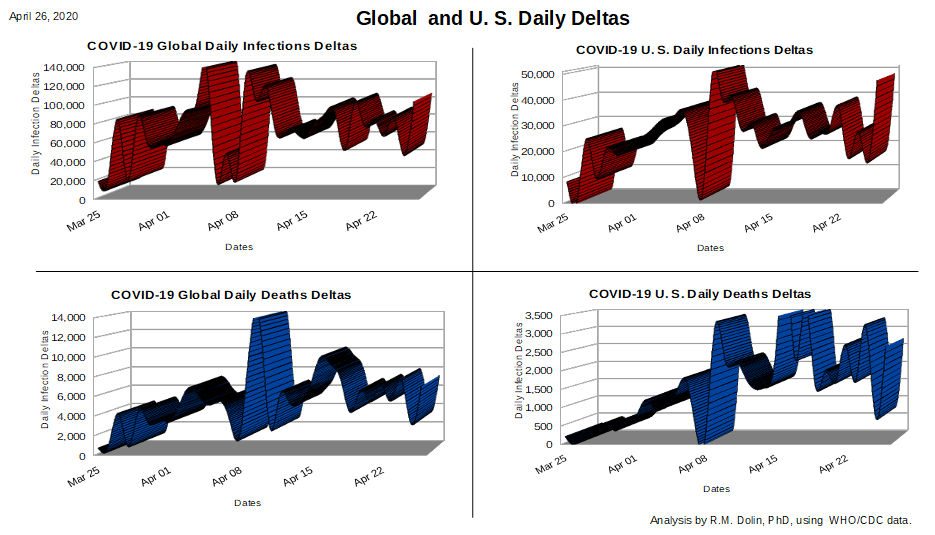
Consider that in America, the COVID crisis is not as bad as past flu seasons; for example, this year’s COVID crisis compared with the 2017 flu season. Can you remember back three years to the many months you spent in quarantine, or the personal liberties you were compelled to surrender? If you can’t, the question is why not? As the table below shows, your likelihood of dying from flu in 2017 was higher than is your likelihood of dying from COVID. Why were the sixty-one thousand flu deaths in 2017 not as precious as the fifty-three thousand COVID deaths in 2020?
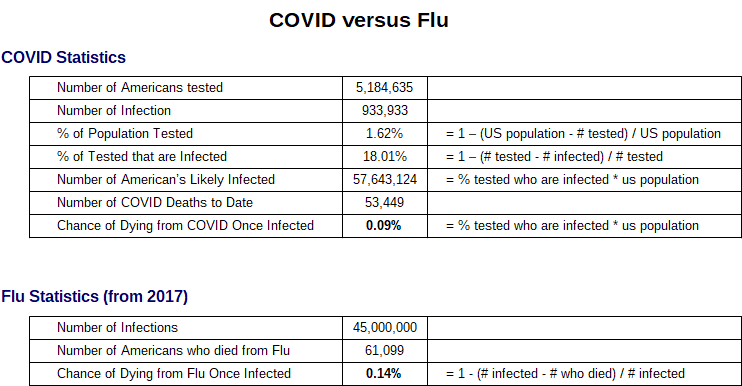
Note about the table and its findings. The number of Americans tested for COVID is based on CDC data, as is the number of infected. Relative to the overall U. S. population, the number tested is small (1.62%), but statistically sufficient enough for a first principles extrapolation to the number of American’s likely infected. This is of course a coarse estimate because it doesn’t take into account mitigating circumstances; such as the population of people tested was not random. The people tested were likely ones who suspected they were infected from particular regions, like New York. But assuming 18% of the population is infected, then the chance of dying once infected is 0.09%. Meanwhile, the chance you would die in 2017 if you got the flu was 0.14%.
Other mitigations that would skew these findings is that the number of COVID deaths is known to be inflated. We’ve previously discussed how New York admits to inflating their COVID death counts by 57%. This week Pennsylvania admitted that they overcounted by 50%. The financial incentive for Doctors and hospitals to overcount, means the true likelihood of dying from COVID once infected, is probably lower than the CDC number shown in the table.
Summary: Throughout history, quarantine has been used to isolate an unhealthy population from a healthy population in order to slow the spread of a disease. Quarantine has never been shown to stop the spread of a disease. During the COVID crisis an inverse-quarantine strategy has been adopted where for the first time in world history, its the healthy population being isolated. A more reasonable and rational approach would be to isolate those who are already sick along with those at high risk, such as people with underlying conditions or genetically predisposed, while letting the healthy population live their normal lives. This is a strategy that has worked going all they back to biblical times.

Comments are closed